»
Danh Mục Bài Viết
»
Kỹ thuật phẫu thuật
»
Danh Mục Bài Viết
»
Kỹ thuật phẫu thuật
Laparoscopic Sigmoid Colectomy (Kỹ Thuật Cắt Đại Tràng Sigma Nội Soi)
Thứ năm - 16/06/2011 15:19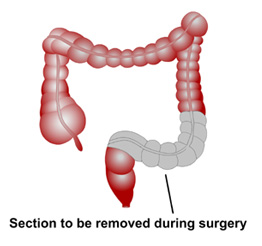
Laparoscopic Sigmoid Colectomy (Kỹ Thuật Cắt Đại Tràng Sigma Nội Soi)
Step 1. The patient is given general anesthesia and placed in the lithotomy position, with a Foley catheter and nasogastric tube (Fig. 1).
Step 2. Usually five trocars are placed in the abdomen as indicated in Fig. 2
Step 3. Place graspers through the trocars in the left abdomen to provide traction on the sigmoid colon. Begin dissection lateral to the sigmoid along the white line of Toldt. We feel that the Harmonic Scalpel is the best instrument for this dissection. This is placed through the port in the right lower quadrant, and a grasper is placed in the right upper quadrant port to facilitate the dissection with counter traction. The dissection can be taken up to the splenic flexure and, if necessary, it can be mobilized (Figs. 3 and 4). We have completely mobilized the splenic flexure using the Harmonic Scalpel and using occasional clips for larger vessels. Distally, the dissection is taken down to the peritoneal reflection. Attention should be given to locating the ureter; this can be facilitated by placing fiberoptic ureteral catheters.
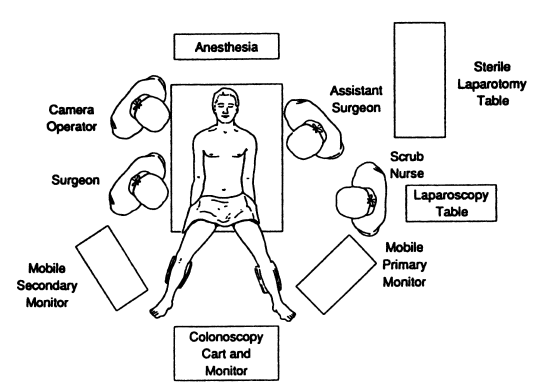
Figure 1. Operating room arrangement for sigmoid resection. (From ME Franklin, Jr. Laparoscopic surgery of colon and rectum. (ME Arregui, RJ Fitzgibbons Jr., N. Katkhouda, JB McKernan, and A Reich (eds.). Principles of Laparoscopic Surgery: Basic and Advanced Techniques. New York: Springer-Verlag, 1995, with permission.)
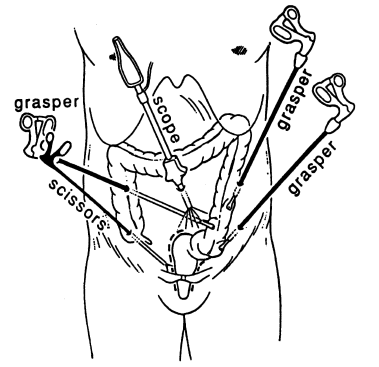
Figure 2. Trocar placement for low anterior and abdominal peritoneal resection. ME Franklin, Jr. Laparoscopic surgery of colon and rectum. (From ME Arregui, RJ Fitzgibbons Jr., N. Katkhouda, JB McKernan, and A Reich (eds.). Principles of Laparoscopic Surgery: Basic and Advanced Techniques. New York: Springer-Verlag, 1995, with permission.)
Step 4. Retract the colon laterally. Again using the Harmonic Scalpel, score the mesentery of the sigmoid colon. Develop a window in the mesocolon and then another window either more proximally or distally. Insert the endoscopic GIA with the vascular staples into the trocar in the right lower quadrant. Then insert it through the windows previously made in the mesocolon, and fire it. Repeat this multiple times until the segment of colon is mobilized.
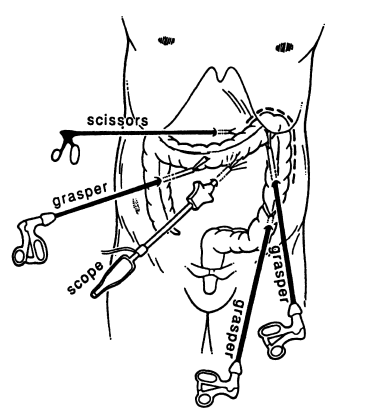
Figure 3. Trocar placement for splenic fl exure and left colon. ME Franklin, Jr. Laparoscopic surgery of colon and rectum. (From ME Arregui, RJ Fitzgibbons Jr., N. Katkhouda, JB McKernan, and A Reich (eds.). Principles of Laparoscopic Surgery: Basic and Advanced Techniques. New York: Springer-Verlag, 1995, with permission.)
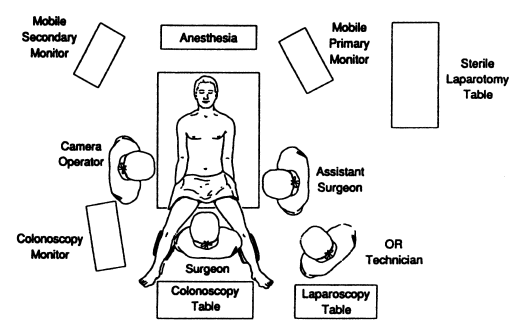
Figure 4. Operating room arrangement for splenic fl exure mobilization. ME Franklin, Jr. Laparoscopic surgery of colon and rectum. (From ME Arregui, RJ Fitzgibbons Jr., N. Katkhouda, JB McKernan, and A Reich (eds.). Principles of Laparoscopic Surgery: Basic and Advanced Techniques. New York: Springer- Verlag, 1995, with permission.)
Step 5. Distally, divide the sigmoid at the peritoneal reflection by inserting the endoscopic GIA through the right lower quadrant trocar.
Step 6. Make a transverse incision about 4–5 cm long in the left abdomen. Remove the sigmoid colon through this incision; transect the specimen and remove it from the field. The anastomosis will be made using an EEA stapler; usually a 29-mm EEA is appropriate but the sizers should always be used to determine the appropriate diameter. Place the anvil of the EEA into the proximal colon, which is then purse-stringed around the anvil-connecting end. With the anvil in place as described, drop the proximal colon into the abdomen; close fascia using a 0 PDS.
Step 7. Grasp the end of the anvil using an instrument made specifically for that purpose. Next, insert the EEA into the rectum and advance it until it is seen gently pushing up against the rectal stump. Slowly turn the knob at the end of the EEA stapler until the point that attaches to the EEA starts to “tent up” the rectal stump. Then push this sharp, cone-shaped end of the EEA through the rectal stump through the center of the staple line. Manipulate the anvil until it snaps onto the EEA. Slowly turn the knob at the end of the EEA, thus approximating the proximal colon and rectum.
Step 8. When they are correctly approximated as indicated on the EEA, fire the device. Open the knob on the EEA one turn, and gently rotate the EEA and remove it from the rectum. One complete doughnut of tissue from the proximal colorectal segment and one from the distal segment should be present in the EEA to indicate a satisfactory anastomosis.
Step 9. Fill the pelvis with water and insert a rigid sigmoidoscope into the rectum for a short distance so as to insufflate the colorectal segment and look for bubbles, which would indicate an incomplete anastomosis. If found, a diverting colostomy should be done. The irrigation fluid is then suctioned out and the pneumoperitoneum is relieved. Remove all trocars and close the fascia at each of the sites with a 0 Vicryl suture. Close the skin with a 4–0 Vicryl subcuticular suture.
Tác giả bài viết: Dr. Ai
Chú ý: bản quyền nội dung thuộc về phauthuatnoisoi.vn
 Xem phản hồi
Xem phản hồi Gửi phản hồi
Gửi phản hồiNhững tin mới hơn
Những tin cũ hơn
ĐĂNG NHẬP
CÁC BỆNH THƯỜNG GẶP
- BỆNH THOÁT VỊ BẸN
Tư Vấn Trực Tuyến
Thống kê truy cập
![]() Đang truy cập :
22
Đang truy cập :
22
![]() Hôm nay :
1120
Hôm nay :
1120
![]() Tháng hiện tại
: 189347
Tháng hiện tại
: 189347
![]() Tổng lượt truy cập : 57522139
Tổng lượt truy cập : 57522139