»
Danh Mục Bài Viết
»
Kỹ thuật phẫu thuật
»
Danh Mục Bài Viết
»
Kỹ thuật phẫu thuật
Laparoscopic Gastrectomy (Kỹ Thuật Cắt Dạ Dày Nội Soi)
Thứ hai - 13/06/2011 13:50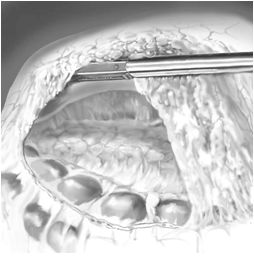
Laparoscopic Gastrectomy (Kỹ Thuật Cắt Dạ Dày Nội Soi)
1. Introduction
Laparoscopic resection of the stomach should mimic an open operation as closely as possible. This is applicable to the technique,as well as to the considerations on which the indication is based. Palliative resection for gastric malignancy can be indicated to preven the morrhageo ro bstruction.
2. Indications and Contraindications
2.1. Indications
■ Malignant tumors [carcinoma, gastrointestinal stromal tumor (GIST)]
■ Benign tumors (e.g., GIST, apudoma)
■ Arteriovenous malformations
■ Recurrent peptic ulcer disease
2.2. Contraindications
■ Severe cardiac failure (unable to with stand pneumoperitoneum)
■ Sepsis
■ Severe coagulopathy
■ Morbid obesity (BMI>40) (relative)
■ Previous upper abdominal surgery (relative)
■ T4 or bulky tumors (relative)
3. Instrumentation
■ Two monitors
■ Three 10 - to 12 -mm trocars, two 5 -mm trocars
■ One 15-mmt rocar( optional) to passthe 60 -mm stapler and retrieval bag
■ 30° laparoscope
■ Unipolar or bipolar coagulation
■ Hemost aticdevice (LigaSure, Ultracision)
■ Standard laparoscopic in struments for advanced laparoscopicsurgery, including fenestrated clampsandendo-Babcock clamp
■ Vascular clip applier
■ Endostapler (45–60mm, withwhite, blue and green cartridges)
■ Liver retractor
■ Vessel loops
■ Gastroscope (optional, to identify small lesions)
■ Retrieval bag
4. Procedure
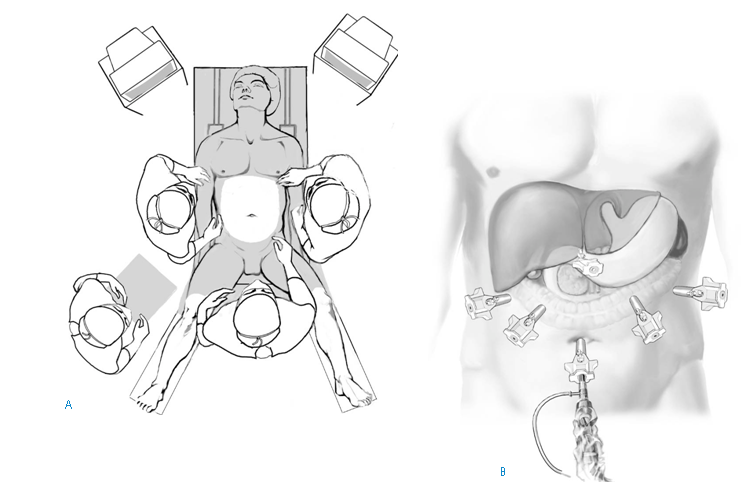
4.1. STEP1: Positioning and installations
Positioning:
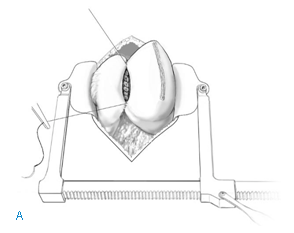
The patient is placed in the supine position. The surgeon stands between the legs of the patient, the first assistant on the left, the second assistant on the right side of the patient. The scrub nurse is positioned on the right or left hand side of the surgeon (A).
Installation of pneumoperitoneum and inspection of abdominal cavity: Pneumoperitoneum is installed at the site of the umbilicus. In obese patients, the umbilicus is located more caudally; in these patients the first trocar may be introduced cranially to the umbilicus. In case of malignancy the abdominal cavity is inspected for signs of dissemination to the peritoneum or other organs. To allow for optimal inspection and to create the opportunity to take biopsies, one or more additional trocars are inserted. Inspection of the caudal side of the mesentery of the transverse colon and the region of Treitz ligament can be facilitated by bringing the patient into a Trendelenburg position.
Introduction of trocars (B): The total number and position of trocars is dependent on the level of resection. The subxiphoidal trocar is only necessary for high resections of the stomach. Introduction of this trocar should be on the left side of the falciform ligament, especially when exploration of the cardia and gastroesophageal junction is necessary.
4.2. STEP2: Opening of the lesser sac
To determine (laparoscopic) resectability of the tumor, opening of the lesser sac is achieved by detaching the greater omentum from the transverse colon by sharp dissection. In case of a benign indication, opening of the lesser sac can be performed more easily by creating a window in the greater omentum, for instance by using Ultracision. Involvement of the pancreas in malignant tumors requires conversion to open resection in most cases. In case of malignancy, once resectability has been established, the lesser sac is opened until the gastrocolic ligament is completely dissected from the hepatic to the splenic flexure.
4.3. STEP3: Resection of benign lesions
In benign lesions, a stapled wedge resection is performed. Resection is performed under gastroscopic surveillance in case the lesion is not visible on the serosal side of the stomach. The gastrohepatic ligament must be opened if the tumor is located on the smaller curvature of the stomach.
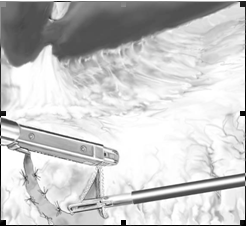
4.4. STEP4: Transection of duodenum and resection of gastrohepatic ligament
After detachment of the greater omentum, the right gastroepiploic vessels are identified and secured with clips at the level of the duodenum.Mayo’s vein will locate the exact position of the pylorus. Identification of the pylorus can be facilitated by gentle palpation with a clamp in the postpyloric area. Care should be taken not to damage the pancreatic parenchyma as this will result in pancreatitis. Sharp dissection at the posterior side of the postpyloric part of the duodenum creates space to introduce a 45-mm stapling device. A vessel loop can be used to facilitate safe insertion of the stapler. Prior to the closure of the stapler, care should be taken that the vessel loo and vascular clips are not included in the line of stapling (A).
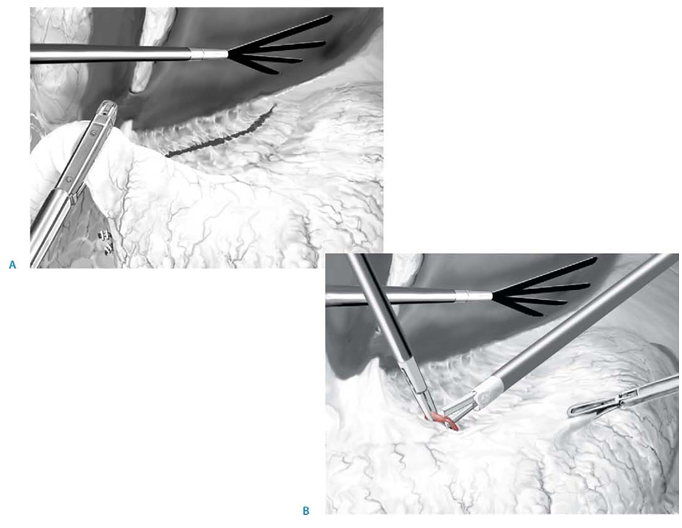
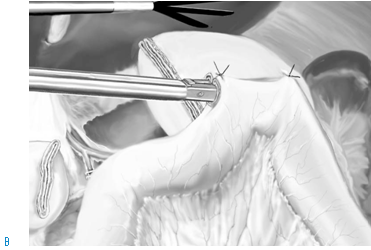
The assistant retracts the liver to allow exposure of the smaller omentum. The gastrohepatic ligament is opened at the level of the hepatoduodenal ligament. The right gastric artery is transected using Ultracision (B). The assistant retracts the liver to allow exposure of the liver hilum. Following the common, proper, and left hepatic artery, the smaller omentum is freed, securing lymph nodes of the pyloric group up to the right pericardial group. This en bloc lymphadenectomy is part of a level D2 resection and is optional. A replaced or aberrant left hepatic artery, originating from the left gastric artery, can be safely dealt with, using clips if necessary. Alternatively this lymphadenectomy can be done after transection of the stomach.
4.5. STEP5: Securing of left gastric vessels
The posterior aspect of the stomach is freed from the anterior surface of the pancreas by sharp dissection of adhesions.At this stage a vessel loop can be used to allow easier manipulation of the stomach. Cranial to the pancreas the splenic artery is identified in most cases.More cranially, the left gastric vessels are identified and transected with
clips or a vascular stapler. Optional D2 lymphadenectomy of the stomach implies truncal lymphadenectomy at this stage.

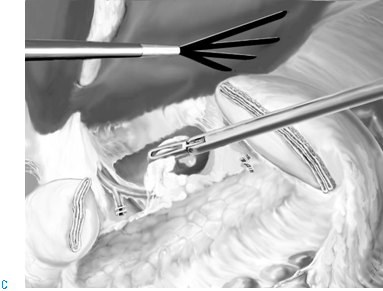
4.6. STEP6: Transection of the stomach
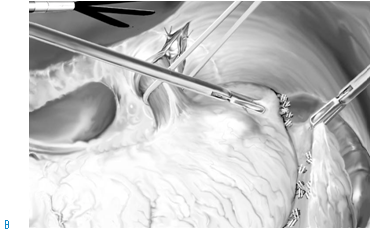
The transection line of the stomach is performed 5cm orally to the tumor (A). If the tumor cannot be identified adequately on the serosal side of the stomach, intraoperative gastroscopy is mandatory to determine the exact line of transection. Location of the tumor high in the body of the stomach may require opening of the gastrosplenic ligament
and securing of short gastric vessels with Ultracision (B).
D2 lymphadenectomy requires resection of lymph nodes of the gastrohepatic ligament and between the hepatic artery. If the nodal clearance has not been performeden bloc, it is feasible to do it at this stage (C).
After transection of the stomach, the specimen is placed in a retrieval bag for safe extraction. Extraction is done through a mini-laparotomy. This laparotomy can be conducted at a cosmetically preferred site (e.g., Pfannenstiehl). Alternatively a midline mini-laparotomy is performed in the upper abdominal region. In the latter option the anastomosis can be done in an open fashion.

4.7. STEP7: Anastomosis
Open anastomosis:
Through a small midline laparotomy a standard Billroth II or Roux-en-Y reconstruction can be performed (A).
Laparoscopic anastomosis (Billroth II):To perform a laparoscopic side-to-side gastrojejunostomy, ligament of Treitz and the proximal jejunum are identified by lifting the transverse colon and tilting the table into a Trendelenburg position (head down). A loop of proximal jejunum is brought up in an antecolic or retrocolic fashion. This loop of jejunum is sutured to the anterior aspect of the stomach remnant with two resorbable, seromuscular stay sutures, approximately 2cm apart. A stab incision in both the stomach and the jejunum is made with diathermia. Care should be taken that the incision in the stomach is made through all gastric wall layers. The stab incisions are enlarged, and the endostapler is introduced with one blade in the stomach and the other in the jejunum. Subsequently the stapler is fired one or two times, dependent on the size of the cartridges (60 or 45mm). In case a 60-mm stapler is used, a 15-mm trocar should be introduced (B).
4.8. STEP8: Closure of stab incisions
The incision that remains in the stomach and the jejunum after firing the endostapler is closed using a single layer resorbable, polyfilament suture. Closure with an endostapler should not be attempted as the anastomosis is easily compromised because it is difficult to ensure inclusion of all tissue of the stomach and jejunum on both sides of the stab incisions in the staple line without narrowing the anastomosis.

5. Postoperative Investigations
Short term:
– Anastomotic insufficiency (including duodenal stump insufficiency)
– Acute pancreatitis
– Chylous ascites (particularly after R2 resection)
Long term (all indications):
– Biliary gastritis (particularly after Billroth II reconstruction)
– Jejunal peptic ulcer disease
Long term (in case of malignancy):
– Local recurrence (duodenal stump or resection line of stomach)
– Distant metastases
Tricks of the Senior Surgeon
Instead of a vessel loop, a heavy resorbable suture can be used to force the stomach or duodenum into the endostapler. Even if this suture is included in he staple line, this will not compromise your anastomosis.
In lean patients it is often possible to remove one of the 10- to 12-mm trocars and directly introduce the 60-mm stapler or the retrieval bag, instead of using
a 15-mm trocar.
Suturing is best done with the scope in the middle and two needle holders on either side of the scope with a 60–90° angle between the two needle holders.
Tác giả bài viết: Dr. Ai
Chú ý: bản quyền nội dung thuộc về phauthuatnoisoi.vn
 Xem phản hồi
Xem phản hồi Gửi phản hồi
Gửi phản hồiNhững tin mới hơn
Những tin cũ hơn
ĐĂNG NHẬP
CÁC BỆNH THƯỜNG GẶP
- BỆNH THOÁT VỊ BẸN
Tư Vấn Trực Tuyến
Thống kê truy cập
![]() Đang truy cập :
16
Đang truy cập :
16
![]() Hôm nay :
1112
Hôm nay :
1112
![]() Tháng hiện tại
: 189339
Tháng hiện tại
: 189339
![]() Tổng lượt truy cập : 57522131
Tổng lượt truy cập : 57522131