»
Danh Mục Bài Viết
»
Kỹ thuật phẫu thuật
»
Danh Mục Bài Viết
»
Kỹ thuật phẫu thuật
Low Anterior Resection, Triple-Staple Procedure (Kỹ Thuật Cắt Trực Tràng Trước Thấp-Nối máy)
Thứ năm - 16/06/2011 11:22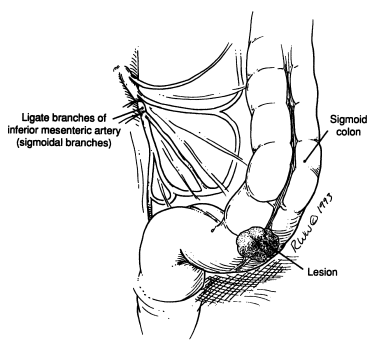
Low Anterior Resection, Triple-Staple Procedure (Kỹ Thuật Cắt Trực Tràng Trước Thấp-Nối máy)
Step 1.
Mobilize the rectosigmoid colon: incise the lateral peritoneal reflection upward to the splenic flexure; incise gently downward to the sacral promontory and the presacral area. Blunt dissection by the surgeon’s hand is advisable (Fig. 1 ).
Remember:
The presacral fascia is part of the endopelvic fascia, without lymphatics, and it is not necessary to remove it. Invasion of the fascia by cancer means it is not curable (Fig. 1 ).
Between the fascia and the presacral periosteum, a network of veins drains into the sacral foramina. To avoid bleeding and injury to the fascia, dissect very close to the posterior colonic wall; bleeding is extremely difficult to stop, even with ligation of both hypogastric arteries. Inserting tacks at the bleeding points is helpful (Fig. 2).
To avoid dysfunction of the urinary bladder, as well as impotence in the male, dissect the left ureter carefully because it travels together with the left hypogastric nerve. Both are located at the posterolateral pelvic wall and hypogastric artery, and the nerve is medial to the ureter (Fig. 1 ).
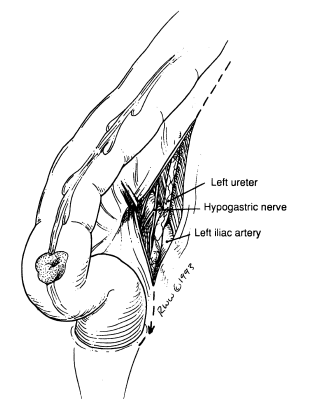
Figure 1

Figure 2
Step 2.
In males, dissect at the prostatic area by dividing Denonvilliers fascia. In females, divide the cul-de-sac and further separate the urinary bladder and vaginal wall from the rectum.
Step 3.
After satisfactory mobilization of the rectosigmoid, ligate the lymphovascular elements as described in the left colon resection and proceed downward for further vascular ligation and further careful rectal detachment, as described above. (Steps may vary depending on sex, local topographical anatomy, and obesity of the patient.)
Step 4.
Place a TA stapler approximately 2–4 cm below the tumor and fire, thus placing a double row of staples across the rectosigmoid. Place an angled bowel clamp proximal to the staple line and divide the colon between the staple line and the bowel clamp (Fig. 3 ).
Step 5.
Place a bowel clamp where the proximal line of excision is to be, divide the colon, and remove the specimen.
Step 6.
The triple-staple technique. This is accomplished by inserting the anvil of the EEA into the proximal colon and then stapling the colon closed with the anvil inside (Fig. 4). The anvil-connecting end, which is cone-shaped and sharp, can then be pushed through the line of staples.

Figere 3
Step 7.
Next insert the EEA into the rectum, and when up against the staple line, begin to turn the knob on the device so that the connector end (also sharp and cone-shaped) will slide through the staple line (Fig. 5 ).
Step 8.
Next the connectors from the anvil and the EEA snap together (Fig. 6 ). The knob at the end of the EEA is then slowly turned, thus approximating the proximal colon and distal rectum (Fig. 7).
Step 9.
When they are correctly approximated as indicated on the dial of the EEA, the device can be fired. The knob on the EEA is then opened one turn and the EEA is then rotated gently and removed from the rectum.
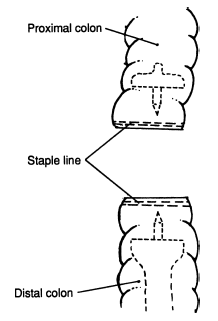
Figure 4

Figure 5
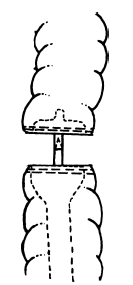
Figure 6

Figure 7
Note:
There should be a complete doughnut of tissue present in the EEA indicating a satisfactory anastomosis. (If the surgeon has any doubt about the anastomosis, a temporary colostomy can be done. One month following the colostomy, a low-pressure Gastrografin enema can be done and, if no leakage occurs, the colostomy can be closed.)
Step 10.
Jackson–Pratt drainage is up to the surgeon. Close in layers.
Tác giả bài viết: Dr. Ai
Chú ý: bản quyền nội dung thuộc về phauthuatnoisoi.vn
 Xem phản hồi
Xem phản hồi Gửi phản hồi
Gửi phản hồiNhững tin mới hơn
Những tin cũ hơn
ĐĂNG NHẬP
CÁC BỆNH THƯỜNG GẶP
- BỆNH THOÁT VỊ BẸN
Tư Vấn Trực Tuyến
Thống kê truy cập
![]() Đang truy cập :
42
Đang truy cập :
42
•Máy chủ tìm kiếm : 4
•Khách viếng thăm : 38
![]() Hôm nay :
1851
Hôm nay :
1851
![]() Tháng hiện tại
: 20272
Tháng hiện tại
: 20272
![]() Tổng lượt truy cập : 57739779
Tổng lượt truy cập : 57739779