»
Danh Mục Bài Viết
»
Kỹ thuật phẫu thuật
»
Danh Mục Bài Viết
»
Kỹ thuật phẫu thuật
Liver: Right Lobectomy(kỹ thuật cắt thuỳ gan phải)
Chủ nhật - 26/06/2011 18:35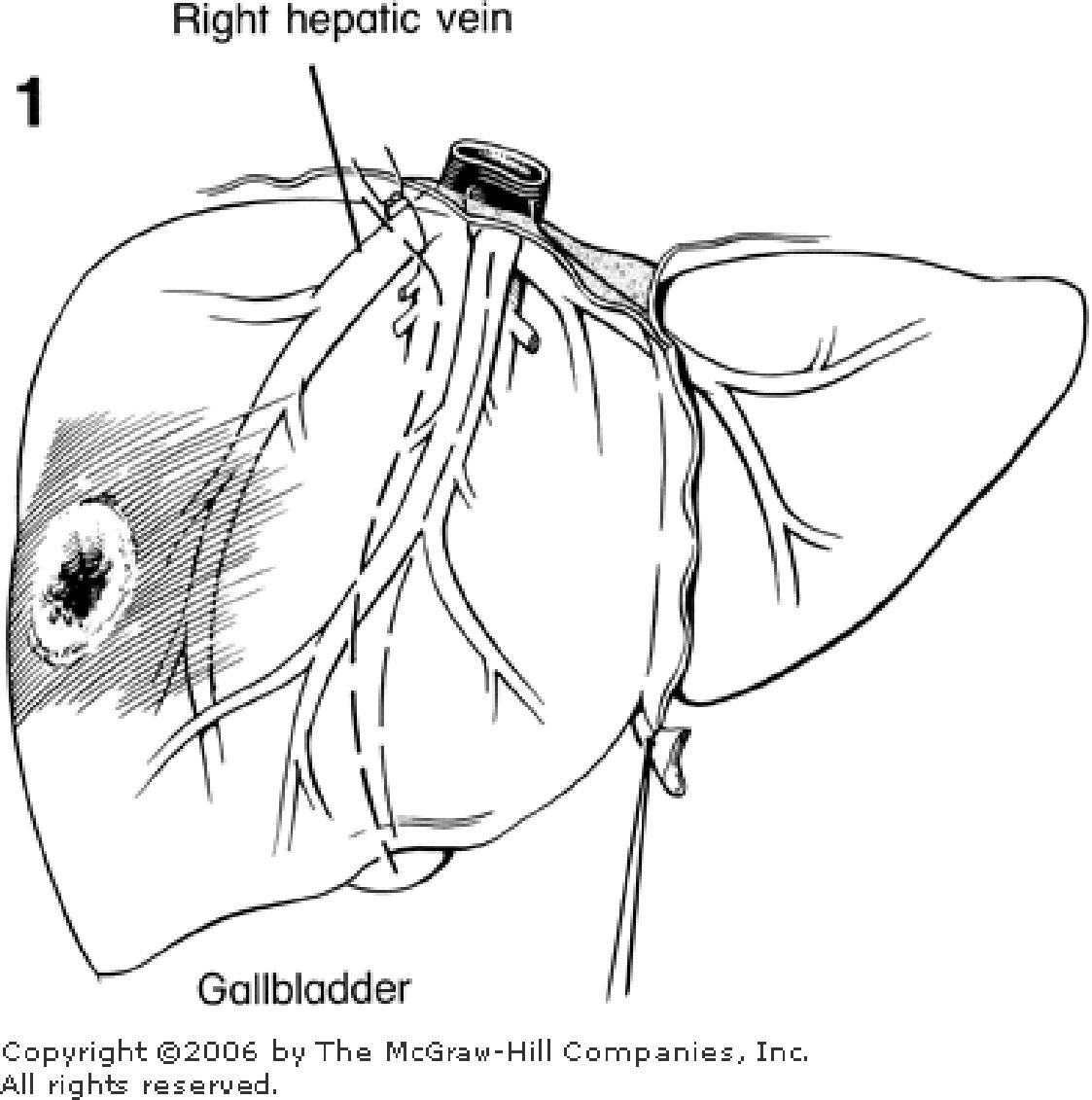
Right Lobectomy
For a right lobectomy or trisegmental lobectomy, a right subcostal incision is used. It may be continued upward into the thorax or to the right if necessary. The right triangular and coronary ligaments are incised so that the right lobe may be retracted. The round and falciform ligaments are preserved. In a “true” right or left lobectomy, the gallbladder must be sacrifi ced. Dissection begins at the hilum. Branches of the hepatic artery, the portal vein, and the bile duct of the lobe to be removed are ligated, and the interlobar hepatic veins are preserved. Blunt dissection must be used throughout. The line of the interlobar fi ssure extends from the gallbladder fossa below to the inferior vena cava above. The dissection must pass to the right of the middle hepatic vein to preserve drainage of the medial segment of the left lobe (Fig. 1 ). The right hepatic vein may be ligated extrahepatically before transection of the liver. A right “extended” lobectomy (trisegmentectomy) is similar, but the liver is transected just to the right of the falciform ligament. The middle hepatic vein must be ligated, since the medial segment is to be removed.
Right Hepatic Lobectomy
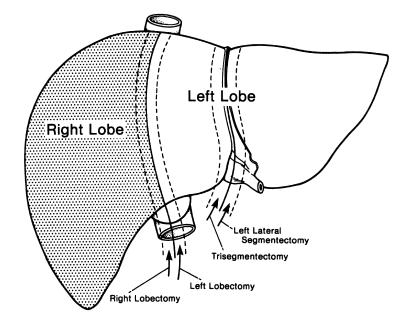
Figure 1
Step 1.
Perform cholecystectomy.
Step 2.
Divide the falciform, right anterior, posterior coronary, and right triangular ligaments. Be careful not to sever the right hepatic vein (Fig. 2 ).
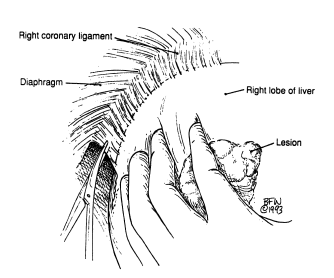
Figure 2
Step 3.
Rotate the right lobe medially.
Step 4.
Identify, isolate, and doubly ligate the right hepatic duct and right hepatic artery. The right portal vein should be treated very carefully with the same technique used in step 5 of the left hepatic lobectomy (Fig. 3 ).

Figure 3
Step 5.
Dissect and carefully prepare the retrohepatic inferior vena cava and its small multiple parenchymal branches, which should be ligated doubly using 4–0 or 5–0 silk (Fig. 4 ).
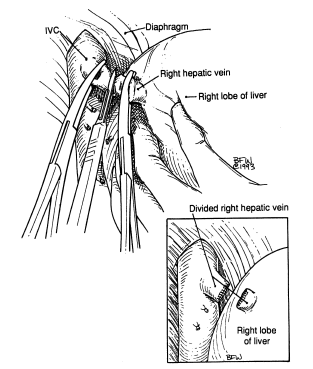
Figure 4
Step 6.
If the right hepatic vein was not ligated previously, it should be dissected very carefully, mobilized, clamped doubly, divided, and oversewn as described in the procedure for left hepatic lobectomy.
Step 7.
If discoloration and demarcation are present between the right and left lobes at this time, divide the two lobes through the previously marked area, as in step 6 of the procedure for left hepatic lobectomy.
Step 8.
For hepatic stabilization, approximate the falciform ligament (Fig. 5 ).
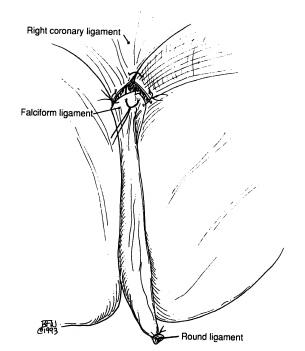
Figure 5
Step 9.
Insert Jackson–Pratt drain.
Tác giả bài viết: Dr. Ai
Chú ý: bản quyền nội dung thuộc về phauthuatnoisoi.vn
 Xem phản hồi
Xem phản hồi Gửi phản hồi
Gửi phản hồiNhững tin mới hơn
Những tin cũ hơn
ĐĂNG NHẬP
CÁC BỆNH THƯỜNG GẶP
- BỆNH THOÁT VỊ BẸN
Tư Vấn Trực Tuyến
Thống kê truy cập
![]() Đang truy cập :
32
Đang truy cập :
32
•Máy chủ tìm kiếm : 1
•Khách viếng thăm : 31
![]() Hôm nay :
1504
Hôm nay :
1504
![]() Tháng hiện tại
: 19925
Tháng hiện tại
: 19925
![]() Tổng lượt truy cập : 57739432
Tổng lượt truy cập : 57739432