»
Danh Mục Bài Viết
»
Kỹ thuật phẫu thuật
»
Danh Mục Bài Viết
»
Kỹ thuật phẫu thuật
Right Colectomy ( Kỹ Thuật Cắt Đại tràng Phải)
Thứ năm - 16/06/2011 09:23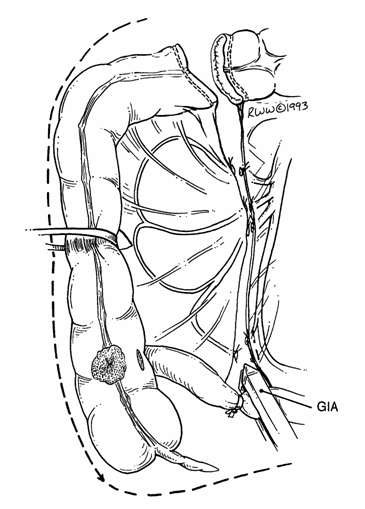
Right Colectomy ( Kỹ Thuật Cắt Đại tràng Phải)
Step 1. As soon as the abdomen is open, decide whether to use the routine or no-touch technique. With the no-touch technique that we prefer, we proceed as follows:
a. Lumina of terminal ileum and transverse colon are occluded with
umbilical tape proximal and distal to the tumor (Fig. 1).
b. Vessels are ligated at their origin (at the superior mesenteric artery or superior mesenteric vein) for complete isolation of the lymphovascular tree (Figs. 1 and 2)
Step 2. Explore the peritoneal cavity, saving until last the vicinity of pathology, i.e., the cecum, ascending colon, or right transverse colon.
Step 3. Make a very superficial incision at the mesentery indicating the line of resection, which should be lateral to the umbilical tape ligatures (Figs. 1 and 2 ).
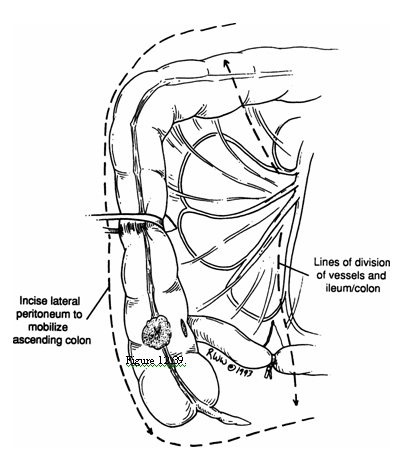
Figure 1
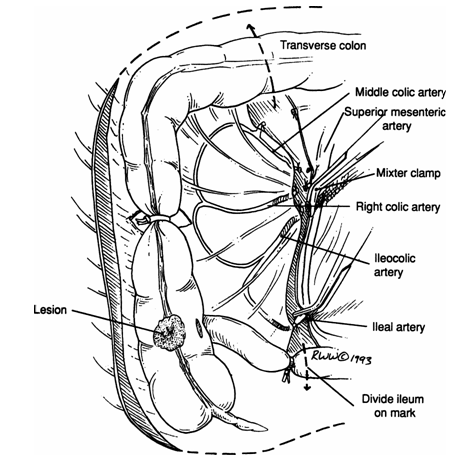
Fgure 2
Step 4. Carefully mobilize the right colon (cecum, ascending, right transverse) by incising the peritoneal reflection of the paracolic area. Elevate the colon with the index finger, protecting the duodenum, right ureter (over the right common iliac artery), and superior mesenteric vessels (Fig. 2).
Step 5. Carry out partial omentectomy, removing the right 3/4 of the greater omentum, including the corresponding part of the gastrocolic ligament, if necessary (Fig. 3).
Step 6. Keeping in mind that occasionally the right colic artery springs directly from the superior mesenteric artery, ligate the two lymphovascular pedicles (ileocolic and middle colic). These ligations should be done carefully to avoid injury to the superior mesenteric vessels as well as to branches of the middle colic supplying the left transverse colon.

Figure 3
Remember:
There are several variations to the anatomy here. Ligate the vessels twice using Mixter clamps.
Step 7. Be sure that both colon and ileum have a good blood supply. We prefer a side-to-side ileotransverse anastomosis using the stapling device. This is done as follows:
a. Division of the ileum by GIA stapler (Fig. 4 ).
b. Division of the colon by GIA stapler (Fig. 4).
c. Align colon and ileum side by side (Fig. 5 ).
d. Partial excision of the antimesenteric corner of the stapled ileal and colonic edges.
e. At the defect, insert the two parts of the GIA stapler, one into the ileal lumen and the other into the colonic lumen. Be sure that the ends of the two parts are at the same point. Fire the instrument. Remove the GIA stapler, inspect the lumina for bleeding, and use the TA stapler to close the triangular areas (Fig. 6). The authors like to reinforce the staple line with a few interrupted 3–0 silk Lembert sutures.
Figure 4
Figure 5

Figure 6
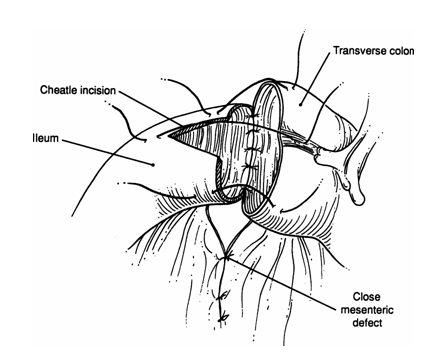
Figure 7
Step 8. Close the mesenteric defect with interrupted 3–0 silk.
Note:
Alternatively, a two-layer end-to-end anastomosis can be done using a running 3–0 chromic for the mucosal layer and interrupted 3–0 silk Lembert sutures for the seromuscular layer (Fig. 7 ).
Tác giả bài viết: Dr. Ai
Chú ý: bản quyền nội dung thuộc về phauthuatnoisoi.vn
 Xem phản hồi
Xem phản hồi Gửi phản hồi
Gửi phản hồiNhững tin mới hơn
Những tin cũ hơn
ĐĂNG NHẬP
CÁC BỆNH THƯỜNG GẶP
- BỆNH THOÁT VỊ BẸN
Tư Vấn Trực Tuyến
Thống kê truy cập
![]() Đang truy cập :
21
Đang truy cập :
21
•Máy chủ tìm kiếm : 2
•Khách viếng thăm : 19
![]() Hôm nay :
1477
Hôm nay :
1477
![]() Tháng hiện tại
: 189704
Tháng hiện tại
: 189704
![]() Tổng lượt truy cập : 57522496
Tổng lượt truy cập : 57522496