»
Danh Mục Bài Viết
»
Kỹ thuật phẫu thuật
»
Danh Mục Bài Viết
»
Kỹ thuật phẫu thuật
Liver Resection and Trauma(kỹ thuật cắt gan trong chấn thương gan)
Chủ nhật - 26/06/2011 19:01
Liver Trauma
In contrast to elective operations on the liver, the surgeon may be faced with traumatic liver injury that does not follow segmental lines. In such cases, the surgeon must decide whether to débride and repair the wound or convert it into an anatomical segmental resection. The problem is that most injuries occur to the right lobe. The choice lies between repair and right lobectomy. If the injury is minor, lobectomy is not justifi ed. If the injury would leave grossly devascularized areas of the liver, then formal lobectomy is necessary. When there is doubt about the severity of the injury but lobectomy is contemplated, operative cholangiograms and aortography can be used to further delineate the area of destruction. In severe trauma there may be no time for angiograms or even for careful hilar dissection. The surgeon must rely on knowledge of the interlobar plane to expose vessels that must be ligated.
Two indications for formal lobectomy have been proposed:
- Blunt or penetrating injuries resulting in extensive devitalization of a major portion of the right lobe
- Damage to the hepatic veins or the vena cava requiring right lobectomy for visualization and repair
Liver Trauma
Step 1.
Make a long midline incision. Suction all blood from the peritoneal cavity.
Step 2.
Mobilize the liver by incising the falciform, triangular, and coronary ligaments on both lobes (Fig. 1 ).
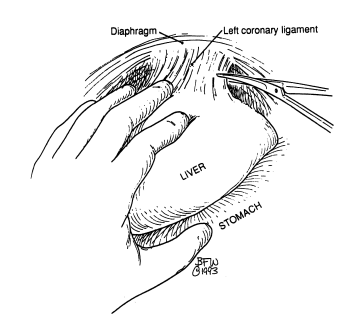
Figure 1
Step 3.
Explore the hepatic wound for evaluation and hemostasis. Débride and remove devascularized liver parenchyma. To control bleeding, it is very helpful to use the argon laser simultaneously with high suction (Fig. 2 ).
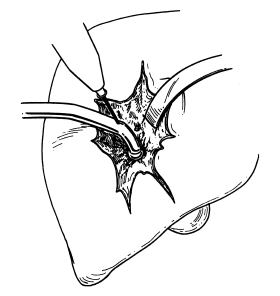
Figure 2
Step 4.
If required, clamp the hepatic triad with a noncrushing clamp (Fig. 3 ).

Figure 3
Step 5.
If bleeding cannot be controlled, ligate the right or left hepatic artery. Perform a cholecystectomy if the right hepatic artery is ligated.
Options or alternatives (use only if absolutely necessary):
- Pack the hepatic wound for hemostasis and re-operate in 48 hours.
- Clamp the aorta just below the diaphragm.
- Isolate the inferior vena cava using Cameron “keepers” (umbilical tape) above the renal veins and within the pericardium. With both ends of the tape threaded into an 18 French catheter, pull them taut by clamping with a Kelly clamp. If this procedure is necessary, a median sternotomy should be performed (Fig. 4 ).

Figure 4
- Occasionally it is necessary to place a shunt into the inferior vena cava. For more details, read the excellent book by John L. Cameron, Atlas of Surgery, vol I. Philadelphia: Decker, 1990.
Tác giả bài viết: Dr. Ai
Chú ý: bản quyền nội dung thuộc về phauthuatnoisoi.vn
 Xem phản hồi
Xem phản hồi Gửi phản hồi
Gửi phản hồiNhững tin mới hơn
Những tin cũ hơn
ĐĂNG NHẬP
CÁC BỆNH THƯỜNG GẶP
- BỆNH THOÁT VỊ BẸN
Tư Vấn Trực Tuyến
Thống kê truy cập
![]() Đang truy cập :
44
Đang truy cập :
44
•Máy chủ tìm kiếm : 1
•Khách viếng thăm : 43
![]() Hôm nay :
1309
Hôm nay :
1309
![]() Tháng hiện tại
: 19730
Tháng hiện tại
: 19730
![]() Tổng lượt truy cập : 57739237
Tổng lượt truy cập : 57739237