»
Danh Mục Bài Viết
»
Kỹ thuật phẫu thuật
»
Phẫu Thuật Mỡ
»
Danh Mục Bài Viết
»
Kỹ thuật phẫu thuật
»
Phẫu Thuật Mỡ
TRI-INCISIONAL ESOPHAGECTOMY (Kỹ Thuật Cắt Thực Quản Mở)
Chủ nhật - 04/12/2011 01:43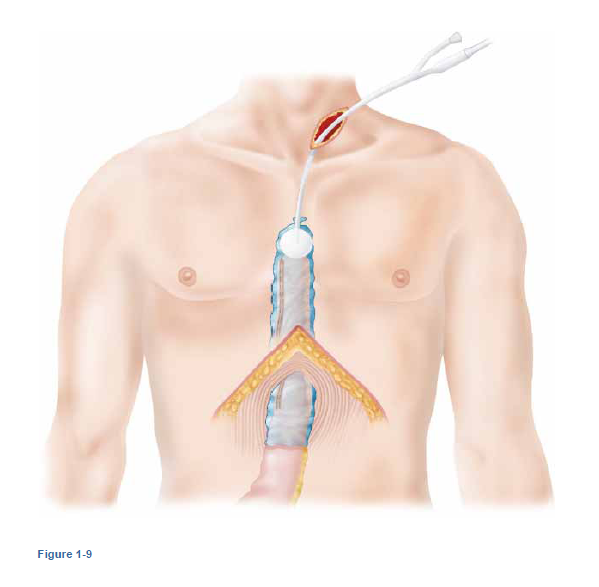
ESOPHAGECTOMY
Step 1: Surgical Anatomy
-The normal stomach will reach the neck when placed in situ in virtually every patient. If a patient has had prior gastric surgery, then it may not reach the neck.
- The upper and mid esophagus are most easily accessed via right-side thoracotomy, as the esophagus deviates to the right and there is no intervening aortic arch.
- The azygous vein crosses the esophagus at approximately the junction of the first third and second third of the esophagus. If the azygous vein is unusually large, it should be preserved. The azygous is infrequently a continuation of an interrupted inferior vena cava.
- The left recurrent nerve loops around the aortic arch and ascends in the tracheoesophageal groove in the chest. The right recurrent nerve loops around the right subclavian artery and ascends in the tracheoesophageal groove. Both nerves are best avoided by keeping dissection inside the vagus nerves above the level of the azygous vein.
Step 2: Preoperative Considerations
- A mechanical bowel prep is wise if there is a possibility of requiring a colon interposition instead of a gastric conduit.
- Preoperative intravenous antibiotics are administered. Although many prefer broad spectrum IV antibiotics, there is no data to show that these are superior to preoperative antibiotics directed only at gram-positive organisms.
- All patients undergoing esophagectomy are at high risk of deep vein thrombosis and pulmonary embolism, and they should receive perioperative subcutaneous heparin and sequential compression devices.
- Patients with limited exercise capacity and risk factors for coronary artery disease (CAD) should undergo cardiac testing prior to operation. Patients with a recent change in cardiac symptoms, change in their EKG, possible aortic stenosis, or signs or symptoms of heart failure should also undergo cardiac evaluation.
- Many factors, including location of tumor, extent of dysplasia, surgeon experience, lung and cardiac function, and patient anatomy factor into the route and method of esophagectomy.
- Patients with bulky mid-esophageal tumors, especially those who have undergone neoadjuvant chemoradiation, are best treated with a transthoracic approach.
- Patients with very poor pulmonary function (i.e., FEV1 <40% predicted) may be better served with a thoracoscopic dissection or transhiatal approach.
- Bronchoscopy with full visualization of the membranous trachea and left main bronchus should be performed by the surgeon for all tumors of the mid and upper esophagus.
- Esophagogastroduodenoscopy must be performed by the surgeon prior to incision.
- A thoracic-level epidural is very useful in managing perioperative pain and minimizing the incidence of pulmonary complications after a thoracotomy.
- The advantages of the tri-incisional esophagectomy include: the complete removal of the esophagus; safe dissection of bulky tumors in the chest under direct vision; and an anastomosis out of the chest.
- Disadvantages include the need for a chest incision, and the higher incidence of recurrent nerve injury with a neck anastomosis.
- Patients with tumors at or above the level of the carina generally require a tri-incisional approach with an anastomosis in the neck.
Step 3: Operative Steps
1.Right Thoracotomy
- The patient is placed in the left lateral decubitus position with an approximate 30-degree forward tilt.
- An abbreviated right posterolateral thoracotomy is performed, starting beneath the tip of the scapula and extending posteriorly 10 cm—typically just long enough to allow introduction of the surgeon's hand.
- The latissimus is divided and the serratus muscle is spared and retracted anteriorly. Entry into the chest is on top of the sixth rib, in the fifth interspace. A 2-cm-long portion of the posterior sixth rib is removed to facilitate spreading of the ribs. The lung is retracted anteriorly and the inferior pulmonary ligament is divided with cautery.
- Starting at a region in the esophagus away from the tumor, the pleura is incised just anterior to the azygous vein. Posterior dissection is performed with a large, blunt right-angle or Harken #1 clamp. Medially, the pleural reflection is taken off the pericardium and dissection proceeds posteriorly. Dissection continues with cautery until a finger can encircle the esophagus, followed by a Penrose drain. All tissue lateral to the pericardium is included in the specimen. (Figure 1-1)
- For tumors at the GE junction, one may choose first to perform dissection in a cranial direction. To the right of the esophagus, all tissue medial to the azygous vein is included in the specimen branches from the aorta are clipped on the aortic side, and cauterized on the esophageal side. All tissue is dissected off the pericardium and included in the specimen. The Penrose drain is used to distract the specimen away from surrounding tissue.
- On the left, the esophagus is dissected off the pericardium, and then away from the left main bronchus. On the right and posteriorly the esophagus is dissected off the aorta, clipping all large branches.
- The anterior vagus nerve is divided at this level, and dissection proceeds in between the vagus nerve and esophagus. (Figure 1-2)
- The posterior (left) vagus nerve is also identified and dissected away from the esophagus.
- The azygous vein is divided with an endovascular 2.5-mm stapler.
- Using low cautery settings, the esophagus is dissected away from the carina and trachea. Some of the dissection may be done using blunt finger dissection.
- The apical portion of mediastinal pleura is preserved in order to minimize the risk of contamination from a cervical leak.
- Dissection at the thoracic inlet is performed bluntly with the fingertip, preserving the apical pleura.
- The Penrose drain is knotted and placed along the cervical spine for retrieval during the cervical phase of the operation.
- Another Penrose drain is placed around the esophagus, and dissection proceeds in a caudal direction.
- Medial dissection removes the esophagus and periesophageal tissue off the pericardium.
- The esophagus is dissected laterally away from the aorta and azygous vein. Large arterial feeders should be clipped on the aortic side.
- Extensive dissection to the right and posterior to the esophagus enters the region of the thoracic duct, but must be performed for bulky tumors.
- For GE-junction tumors, a rim of diaphragm is included in the specimen. The rim is elevated away from intraabdominal structures using a large right-angle clamp.
- Mass ligation of the thoracic duct is performed at the level of the esophageal hiatus.
- The pleura overlying the vertebral body lateral to the aorta is incised.
- A blunt-tipped right-angle is used to encircle all tissue anterior to the vertebral body and aorta.
- A #1 silk ligature is used to tie the tissue; take care not to tie too tightly, which could tear through the duct. (Figure 1-3)
- A suture ligature can be performed, but there may be a higher risk of lacerating the duct.
- The Penrose is knotted and placed into the abdomen for retrieval during the abdominal phase of the operation.
- An examination of the esophageal bed is made for bleeding or for leakage of clear fluid, which may be an indication of a thoracic duct tear in the unfed patient.
- A 28 straight chest tube is placed to the right apex with an additional hole cut to drain fluid from the right pleural base.
- The chest is closed with #1 or #2 Vicryl paracostal sutures.
- Latissimus is reapproximated with a running 0 Vicryl suture.
- The subdermal layer is closed with a running 2-0 Vicryl suture.
- The subcuticular layer is closed with a running 3-0 monocryl or Vicryl suture.



2.Laparotomy
- A midline upper laparotomy is performed from the base of the xiphoid process to 2 cm above the umbilicus. If the xiphoid process is excessively large, it can be excised.
- The omentum, liver, and serosal surfaces of the abdomen are explored for metastatic disease. If preoperative suspicion of abdominal metastatic disease is high, as in patients with celiac adenopathy, minimal response to neoadjuvant therapy, or signet cell pathology, a laparoscopy should be performed as the initial step. The right gastroepiploic artery is palpated—the pulse should be strong.
- An upper hand retractor is placed at about the level of the nipples. A Balfour retractor is used in addition to the upper hand retractor. Alternatively an Omni-type retractor can be used as the sole retractor. The patient is placed in a reverse Trendelenburg position.
- The attachments between the left lobe of the liver and the diaphragm are divided, taking care not to injure the left hepatic vein. The left lobe of the liver can be folded downward and retracted if the lobe is thin, taking care not to lacerate the surface of the liver. If the left lobe of the liver is thick, then it should be elevated anteriorly.
- Cautery is used to enter and divide the clear areas of the gastrohepatic ligament. An ultrasonic scalpel can be used for thicker areas of the ligament. Dissection proceeds up to the right crus.
- If a Penrose drain has been placed during the thoracic phase of the operation, it is now located and grasped. If not, a rim of diaphragm is included with the esophagus at the hiatus, with care to suture ligate the phrenic vein, which crosses anteriorly.
- At approximately the midpoint of greater curvature, entry is made into the lesser sac, several centimeters away from the gastroepiploic artery. Cranial dissection proceeds with cautery through clear areas, and with ultrasonic scalpel or with clamping and ligation through areas with thicker tissue. The surgeon to the patient's right side grasps the greater curvature of the stomach (with care not to compress or manipulate the right gastroepiploic artery) and retracts medially. The surgeon to the patient's left side uses one hand to keep abdominal contents away from the area of dissection and the other hand to distract tissue laterally.
- Dissection proceeds along the greater curvature with care to stay at least 2 cm away from the gastroepiploic artery. The artery eventually ends, and the lateral arcades supplying the stomach become short gastric arteries.
- The anterior and posterior leafs of the short gastrics may be divided with the ultrasonic scalpel, or may be divided with sequential firings of the endoscopic stapler (2.0-mm-thick staples). Often the highest short gastrics enter the cardia of the stomach immediately adjacent to the left crus. Dissection into the splenic artery or pancreas must be avoided. Dense adhesions in this area may make dissection difficult.
- Typically there are loose adhesions between the posterior aspects of the stomach and pancreas, which are divided with cautery.
- The stomach is retracted anteriorly, and the pedicle of the left gastric artery is identified. Sharp dissection with blunt-tip scissors or with cautery is used to dissect all nodes at the origin of the left gastric artery and sweep them onto the specimen. Celiac nodes can also be dissected in this fashion (Figure 1-4) The base of the left gastric artery is clamped with an endovascular stapler that is 45 mm in length and 2.5 mm in height. The right gastroepiploic artery should be palpated at this point to insure that the celiac axis has not been clamped and the stapler is fired. (Figure 1-5)
- At this point dissection proceeds along the greater curvature of the stomach toward the pylorus.The gastroepiploic artery may wander away from the greater curvature of the stomach in this location.
- A Kocher maneuver is performed by retracting all abdominal contents to the patient's left side. Any adhesions between the gallbladder and duodenum are lysed. The duodenum is found at the pylorus and followed to where it attaches to the retroperitoneum. The highest peritoneal attachments are incised with scissors. The surgeon's index finger may then be introduced behind the lateral attachments, and cautery on the index finger will release the attachments. Gentle blunt sweeping of the duodenum medially can be performed with the surgeon's finger or a sponge stick. The medial blood supply to the duodenum must be preserved.


3.Cervical and Laparotomy Phase
- An incision is made from the sternal notch to the level of the cricoid cartilage, anterior to the border of the left sternocleidomastoid muscle (about 6 cm). The platysma is divided with cautery. The omohyoid may be divided with cautery if it interferes with access to the esophagus.
- A self-retaining retractor may be used, but the medial blades should be placed against the skin and platysma, and must not rest in the tracheoesophageal groove.
- Blunt dissection is performed with the two index fingers medial to the jugular sheath and lateral to the trachea down to the vertebral body. The prevertebral plane is entered, the knot in the Penrose drain is palpated, and the Penrose drain is brought up into the wound.
- Additional gentle blunt dissection may be performed to obtain additional proximal length on the esophagus.
- The nasogastric tube is withdrawn, a GIA stapler (35-mm height) is applied across the esophagus,and a heavy, 36-inch stitch is attached to the specimen side. The stapler is fired, and the specimen and stitch are brought into the abdomen. A snap is placed on the end of the suture remaining in the neck.
- A snap is placed on the end of the suture in the abdomen.
- At a point on the lesser curvature near the crow's foot of veins, the right gastric artery and surrounding tissue are dissected free and ligated or divided with an endovascular stapler.
- The gastric tube is created: At a point on the greater curvature approximately 6 cm from the edge of tumor, thick-tissue (48 mm in height) GIA 80-mm staplers are applied parallel to the greater curvature of the stomach. A conduit width of at least 5 cm is desirable to allow for adequate conduit emptying. (Figure 1-6)
- Care is taken to insure that excess gastric tissue does not “bunch-up” in the stapler; excess room is left at each end of the stapler during each fire. Sequential firings of the thick-tissue stapler are performed taking care to align the staple lines. Three to five firings may be needed. (Figure 1-7)
- At this point in time, the specimen is sent to pathology for margins.
- The overlapping areas of the thick-tissue stapler firings on the lesser curve of the stomach are oversewn with imbricating 3-0 silk sutures. Large short gastric stumps are tied with 3-0 silk ties, with care not to incorporate the gastric wall.
- A pyloroplasty or pyloromyotomy, is performed at this point, if the surgeon chooses so. Some surgeons prefer a pyloromyotomy, but are prepared to convert to a pyloroplasty if the lumen is entered. If a pyloroplasty is performed, a right angle clamp is used to elevate the anterior portion of the gastric and duodenal wall away from the posterior wall aids in visualizing the mucosa and in avoiding closing the anterior and posterior walls together.
- Prior to bringing the conduit into the chest and neck, inspection for hemostasis is made in the bed of the mobilized stomach.
- One atraumatic method of bringing the conduit into the neck involves an endoscopic camera bag. A 30-cc Foley balloon is placed into a laparoscopic camera bag, and the bag is tied around the Foley using heavy silk suture. The balloon is filled with saline. The long heavy silk ligature traversing the chest is attached to the valved end of the Foley and is brought into the neck.
- The conduit is placed into the bag, properly oriented so that the staple line is on the patient's right side. Suction is applied to the drainage port of the Foley and the assistant draws the Foley up into the neck. The surgeon on the right side of the abdomen grasps the bag containing the tip of the conduit and guides it up into the chest, until the pylorus lies at the hiatus. (Figures 1-8 and 1-9)
- The bag is opened in the neck and a Babcock instrument is used to grasp the tip of the stomach.
- A corner of the esophageal staple line is cut off with scissors. Cautery is used to make a 1-cm hole in the gastric conduit opposite the staple line. The entrance into the gastric conduit should be placed at a distance from the staple line to minimize ischemia.
- One limb of a GIA 80 mm 35 mm in height stapler is placed in the esophagus and the other limb is placed into the gastric lumen. The stapler is fired to create the anastomosis. As the stapler is separated and withdrawn, the staple line is inspected for hemostasis. The nasogastric tube is passed with its tip verified at the pylorus, and the enterotomy site is closed with either 3-0 interrupted silk sutures or a TA 60 thick-tissue stapler. (Figure 1-10ABC)
- A Penrose or JP drain is placed posteriorly along the spine, and the platysma is closed with interrupted suture. The skin is closed with staples.
- After the creation of a J-tube, the abdomen is closed with running looped #1 PDS or Prolene and staples for the skin.





Step 4: Postoperative Care
- The chest tube can be removed when the drainage is about 200 cc per day, usually by postoperative day 2 or 3. There is little merit to leaving the chest tubes in until a swallowing study is done—intrathoracic leaks generally require immediate reoperation.
- The epidural is generally left in place until after the chest tube is removed and the patient is tolerating enteral narcotics (typically 5 to 6 days).
- Typical presenting symptoms of chyle leaks are high chest tube output (500 cc to 1 L or more per day) that persists after postoperative day (POD) 2. The fluid may be clear but turns milky white after feeding the patient with several hundred mls of heavy cream via J-tube. Treatment is mandatory. If the duct is found to be large during an MRI, then percutaneous fenestration and/or coiling of the duct is an effective treatment. Reoperation with mass ligation (or re-ligation) of the duct at the hiatus and suture of the duct injury with fine Prolene and pledgets is the standard treatment. Instilling 200 cc of cream into the J-tube several hours prior to the operation helps with identifying the site of the leak.
- The neck drain is typically left until after the swallow is performed. A barium swallow will miss 10% of cervical leaks. The patient is then asked to drink grape juice (its purple color is not confused with serosanguineous drainage). If no purple fluid is seen in the drain, then it is removed.
- Recent publications have shown that the pulmonary complications are the main contributors to mortality following esophagectomy.
- One must be vigilant to recognize recurrent nerve injuries. These typically present with hoarseness or a soft voice, and an ineffective cough. This may not present until postoperative day 2 or 3 when cord swelling from double lumen tube intubation and fluid administration subsides. A patient with a recurrent nerve injury may also be at increased risk of aspiration. Immediate medialization of the cord (usually by injection) will improve the voice and cough and allow for effective clearance of pulmonary secretions. Occasionally, a patient with a recurrent nerve injury may still have an effective cough. If so, treatment may be deferred if a video swallow shows no increased risk of aspiration.
- Patients undergoing esophagectomy are at extremely high risk for DVT and PE. They should have sequential pneumatic compression boots applied and subcutaneous heparin administered upon induction of anesthesia.
- Postoperative hypotension is not uncommon, especially with the use of epidurals, and should be treated with aggressive and generous volume administration and not pressors. Generally by postoperative day 2-3 intravenous fluids can be stopped and diuresis begun.
- Extreme vigilance must be maintained for signs or symptoms of conduit necrosis or leak. Unexplained fever, tachycardia, leukocytosis, or pleural effusion should raise suspicion. A base deficit can be a sign of conduit hypoperfusion, but is nonspecific and common after esophagectomy for the first 12 to 24 hours.
- Patients should be maintained with the head of bed elevated 30 degrees or greater to minimize the risk of aspiration pneumonia.
- Ambulation starting on POD1 helps prevent DVT and speeds recovery. Epidurals, chest tubes, oxygen, and Foley catheters should not anchor a patient to their bed.
- Low-dose beta blockade (metoprolol 5 mg IV q4h) is useful in preventing atrial fibrillation, and in controlling the rate should fibrillation occur.
- Tube feeds are begun after flatus at 30 cc per hour at full strength and advanced at 10 cc/hr every 12 hours. Some choose to begin tube feeds prior to evidence of return of bowel function, with care to watch for abdominal distension and avoid ileus with duodenal distension. An ileus in an esophagectomy patient can easily lead to aspiration pneumonia.
- Patients are typically discharged on full liquid diets for 1 to 2 weeks until anastomotic swelling resolves. They can then advance to soft solid food.
Step 5: Pearls and Pitfalls
- At the level of the azygous vein, the vagus nerves should be identified and detached from the esophagus. Cranial dissection proceeds within the vagus nerves.
- Cautery must be done carefully along the course of the trachea and at low settings in order to avoid delayed tracheoesophageal fistula or left recurrent nerve injury.
- During mobilization of the stomach, the surgeon must be vigilant about preservation of the gastroepiploic vascular arcade. Excessive handling, manual compression, thermal injury, and suture injury can turn a routine operation into a life-threatening event. In the obese patient the artery may be difficult to see and its location should be continually reassessed.
- The highest and largest short gastric arteries should be tied on the gastric side in order to avoid postoperative bleeding. It is usually easiest to do this after completion of the gastric tube after initially dividing the short gastrics with an ultrasonic scalpel. Simple use of an ultrasonic scalpel or clips may be inadequate. The ties must not incorporate gastric wall—delayed necrosis and perforation may result.
- Unlike most applications of staplers, the creation of the gastric tube with the GIA thick-tissue stapler requires great care. Excess tissue must not bunch up into the stapler. Successive applications of the stapler should be carefully aligned. The point of intersection of successive staple lines should be imbricated with silk sutures.
- When the conduit is passed through the chest up into the neck, it must be guided through the hiatus from below. Correct orientation must be insured so that the conduit does not twist 180 degrees.
Khám ung thư thực quản ở đâu?
Tác giả bài viết: Dr. Ai
Chú ý: bản quyền nội dung thuộc về phauthuatnoisoi.vn
 Xem phản hồi
Xem phản hồi Gửi phản hồi
Gửi phản hồiTheo dòng sự kiện
Những tin mới hơn
Những tin cũ hơn
ĐĂNG NHẬP
CÁC BỆNH THƯỜNG GẶP
- BỆNH THOÁT VỊ BẸN
Tư Vấn Trực Tuyến
Thống kê truy cập
![]() Đang truy cập :
84
Đang truy cập :
84
•Máy chủ tìm kiếm : 1
•Khách viếng thăm : 83
![]() Hôm nay :
908
Hôm nay :
908
![]() Tháng hiện tại
: 265031
Tháng hiện tại
: 265031
![]() Tổng lượt truy cập : 48074899
Tổng lượt truy cập : 48074899