»
Danh Mục Bài Viết
»
Kỹ thuật phẫu thuật
»
Phẫu Thuật Mỡ
»
Danh Mục Bài Viết
»
Kỹ thuật phẫu thuật
»
Phẫu Thuật Mỡ
Liver: Left Lobectomy(kỹ thuật cắt thuỳ gan trái)
Chủ nhật - 26/06/2011 01:55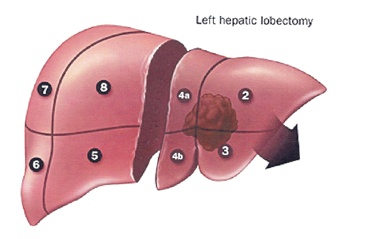
Liver
If the left lobe is to be resected, the left hepatic artery, the portal vein, and the bile duct should be ligated. Section of the triangular ligament will permit mobilization of the left lobe. Transsection should follow a line from the left side of the fossa of the gallbladder to the left side of the fossa of the inferior vena cava (Fig. 1 ). The left and middle hepatic veins should be exposed and ligated within the liver. In most cases, the left and middle hepatic veins form a common trunk before emerging from the liver. It is best to ligate the hepatic veins at the end of the dissection to be sure that only the veins from the resected segments are ligated. A left resection may be lobar, segmental, or even wedge-shaped for a superfi - cially located tumor.
Left Hepatic Lobectomy
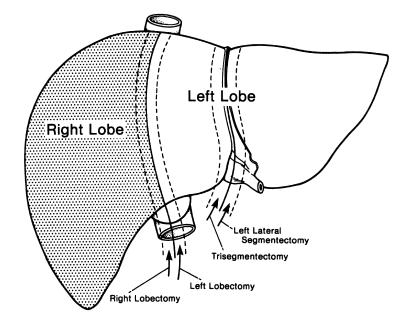
Figure 1. Planes of transection of the liver for lobectomy and segmentectomy. Trisegmentectomy includes the anterior and posterior segments of the right lobe and the medial segment of the left lobe. (By permission of JE Skandalakis, SW Gray, and JR Rowe. Anatomical Complications in General Surgery. New York: McGraw-Hill, 1983.)
Step 1.
Perform cholecystectomy.
Step 2.
Carefully dissect and isolate the left hepatic duct, left hepatic artery, and left portal vein (Fig. 2 ).
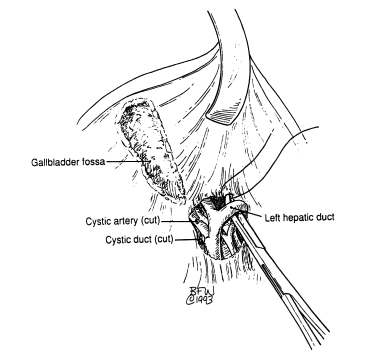
Figure 2
Step 3.
Divide the left triangular, left coronary, and falciform ligaments (Fig. 3 ).
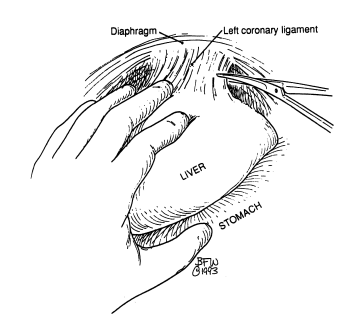
Figure 3
Step 4.
With 2–0 silk, doubly ligate the left hepatic duct and left hepatic artery. The left portal vein should be clamped proximally and distally and, after division, oversewn with 5–0 synthetic nonabsorbable suture or silk (Fig. 4 ).
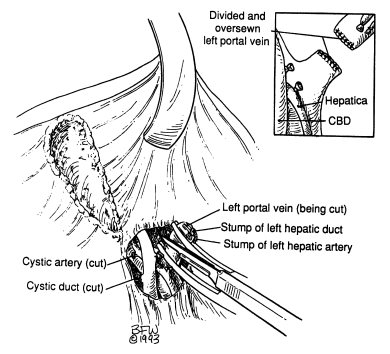
Figure 4
Step 5.
Prepare and isolate the left hepatic vein. Clamp, divide, and oversew the vein as described in step 4 for the left portal vein. If the left hepatic vein is intrahepatic, proceed with lobar division (Fig. 5 ).

Figure 5
Step 6.
By very superficial electrocoagulation, indicate the line of Rex on the Glisson’s capsule of the liver. Start division of the hepatic parenchyma using the CUSA (Cavitron ultrasonic aspirator), and ligate vessels and ducts with 0 or 2–0 silk (Fig. 6 ). Further hemostasis is obtained with the argon laser.
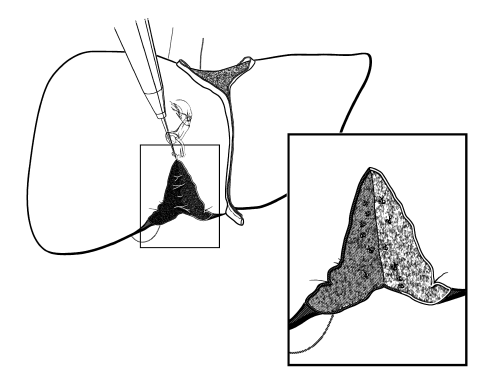
Figure 6
Step 7.
Insert Jackson–Pratt drains.
Step 8.
Close abdominal wall in layers.
Left Lateral Segmentectomy (Fig. 8)
Step 1.
With scissors, carefully section the right triangular and coronary ligaments (Fig. 3 ). Be sure to avoid injuring the left hepatic vein.
Step 2.
With the electrocautery, score the line of resection 1–1½ cm lateral to the falciform ligament (Fig. 7 ).
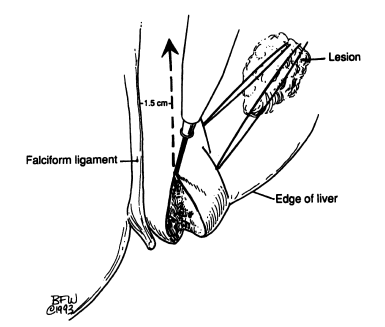
Figure 7
Step 3.
Proceed as in step 6 of left hepatic lobectomy (above).
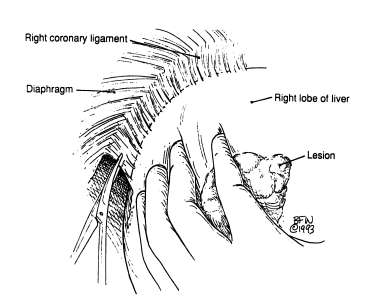
Figure 8
Tác giả bài viết: Dr. Ai
Chú ý: bản quyền nội dung thuộc về phauthuatnoisoi.vn
 Xem phản hồi
Xem phản hồi Gửi phản hồi
Gửi phản hồiNhững tin mới hơn
Những tin cũ hơn
ĐĂNG NHẬP
CÁC BỆNH THƯỜNG GẶP
- BỆNH THOÁT VỊ BẸN
Tư Vấn Trực Tuyến
Thống kê truy cập
![]() Đang truy cập :
146
Đang truy cập :
146
•Máy chủ tìm kiếm : 16
•Khách viếng thăm : 130
![]() Hôm nay :
30831
Hôm nay :
30831
![]() Tháng hiện tại
: 712717
Tháng hiện tại
: 712717
![]() Tổng lượt truy cập : 48522585
Tổng lượt truy cập : 48522585